









Is talk therapy enough for addiction issues?
I have been a licensed marriage and family therapist for years. During that time I found “talk therapy” to be less than successful with many clients, who tended to say what they thought I wanted to hear, framed situations to their advantage, and lied about certain issues. Behavior didn’t change and lives didn’t improve.
John Grinder and Richard Bandler, developers of Neurolinguistic Programming (NLP), identified strategies for effectively questioning clients’ perceptions and guiding them in making those changes. I will introduce several of these strategies and discuss a scenario, which demonstrates how to use them with a client wishing to remain drug-free after completing a treatment program.
Then, I invite you to ask questions regarding NLP and the treatment of addictions at the end. But first, let’s quickly review the basics of NLP.
What is Neuro Linguistic Programming?
NLP examines the fundamental dynamics between the mind (neuro) and language (linguistic); as well as, how their interaction affects the body and behavior (programming).
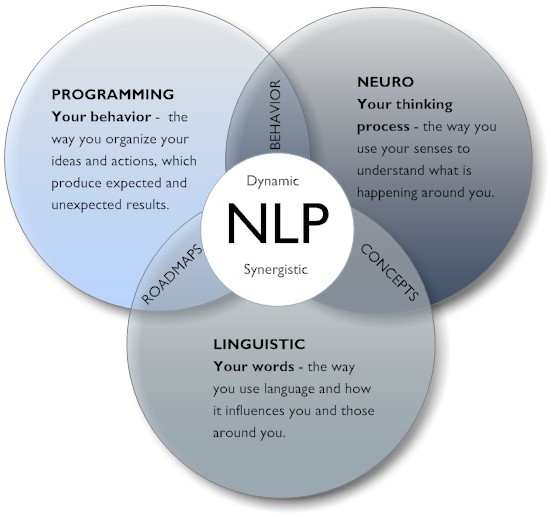
It targets how people:
- communicate externally and internally
- process, store, and recall information
- can alter their communication to achieve the results and goals they want – in this case, overcoming an addiction
Practitioners believe human beings have an extraordinary capacity for flexibility, and there is nothing which happens on a mental or spiritual level they cannot learn to handle. The focus is on how individuals structure their thoughts as they move toward a behavior or motivation – for our purposes, thoughts that lead a person to use substances and those that lead to healthier choices.
NLP strategies that apply to addiction treatment
While NLP can be used by a counselor working with a client experiencing addiction issues, by families with a loved one overly involved with substances, or by an individual who is abusing drugs; we are focusing on strategies for treating clients. I firmly believe that a single method does not work for every client or that the same method will work with a client every time. Therefore, I have developed a “backpack of possibilities” which includes the following strategies.
1. Outcome Specification
This process is a way of clarifying goals and desires. Knowing what the client truly wants to achieve helps the counselor find a purpose-driven course of action and clarify which courses of action are not necessary.
2. Association and Dissociation
A memory or emotional state can be accessed from within (association) or as an observer (dissociation); both are useful. When a person wants to capture an effective way of being, like feeling confident, recalling a time when he or she experienced confidence can enable a reproduction of the feeling in the present. Conversely, when the goal is to put distance between self and an unpleasant memory, viewing it in a disassociated way – as if watching a movie – helps lessen the emotion.
3. Accessing Clues and Predicate Phrases
Typically, accessing clues refer to eye movement. They indicate the sensory representational system a person is using – visual, auditory, or kinesthetic – as they attempt to gain access to information. However, voice tone, breathing patterns, and posture also provide clues. Once the clues are understood, rapport can be built by matching a client’s preferred style of thinking: using words which match the representational style like “I see what you mean” for visual retrievers or “I hear what you say” for auditory retrievers.
Similarly, visual, auditory, kinesthetic and auditory wording, known as predicate phrases, offer clues to a person’s preferred representational system. Comments such as “see what I mean” or “sounds good” provide information.
4. The META Model and the MILTON Model
Given that most people have a tendency to speak in shorthand, the Meta Model provides a way of finding out what is not being said – helping to identify and transform problematic vagueness. The model was designed to deconstruct the way a problem is worded to get to the bottom of it.
Conversely, The Milton Model is deliberately, artfully vague; allowing a person the freedom to interpret what is being said in a way that has meaning for him or her personally.
5. Chunking Down
In NLP, the term “chunking down” refers to a process of moving to details and specifics and “chunking up” refers to a process of moving to abstractions and conceptualizations. Chunking is also a way of breaking a large task into smaller, more manageable ones.
6. Anchors
Anchors are stimuli that trigger specific physiological or emotional states or behaviors – an automatic reaction to something. They can occur unintentionally (like a song evokes memories of an old friend) or created intentionally (by pinching the ear when feeling very confident, so that pinching the ear triggers that desired feeling when needed).
7. Logical Levels
While Gregory Bateson, an outstanding scientist and philosopher, developed the notion that natural hierarchies occur in a person’s thinking, learning, and communication processes, Robert Dilts, an expert in the field of NLP, furthered the concept. Logical Levels are used for organizing thinking, information gathering, and communicating – helping establish an understanding of what makes a person “tick”. When looking for reasons why change is not occurring, it can be helpful to determine exactly where a block is located and where it would be most effective to intervene. The five levels of experience from lowest to highest are:
- Environment – what is around us
- Behavior – what we do
- Capability – what we are able to do
- Belief – what we think we can or should do
- Identity -what we think we are
8. Six Step Reframe
This traditional NLP process is used to improve unwanted behavior. Behavior can be changed by identifying the part of the mind influencing it, determining the positive intent of the behavior, and engaging the creative part of the mind to find better ways to meet the same purpose. The steps are as follows:
- Identify the problem behavior.
- Determine the positive intention behind the behavior.
- Conditionally close with the question “If there were other ways of accomplishing this positive intention, would the client be interested in discovering them?”
- Brainstorm new ways to accomplish the positive intention.
- Identify a minimum of three new choices from the list.
- Conduct an Ecology Check – considering whether or not the new choices feel comfortable.
9. Strategies
This technique suggests thoughts are sequential in nature, a person thinks about one thing, and then another leading to an outcome or to motivation. These thoughts are formulated based on visual (V), auditory (A), kinesthetic (K), olfactory (O), or gustatory (G) information. The purpose of the strategy is to determine how a person composes the VAKOP phenomenon on his or her way to the results they experience. The first step is to evaluate what sensory input is involved and in what order. Once that is known, changes can be made to elicit more adaptive patterns.
CASE STUDY: a client addicted to pain killers
Josie is the 34 year old mother of 4 boys; ages 2 to 8. Her Marine husband has been overseas for 6 months on his third deployment. A year ago, she had back surgery and was prescribed pain medication; however, the pain remained. The doctor prescribed a stronger medication and, then, a combination of medications. Before long, Josie was buying them online when she could no longer get her prescription re-filled.
Quickly, she became addicted to pain-killers both physically and psychologically. When her family realized the depth of the problem, they admitted her to a three-week drug treatment program. During the program, aspects of the addiction were addressed and the physical symptoms were resolved – her body no longer craved the pain-killers; however, emotional ties remained. Josie felt stronger but didn’t want to relapse; so, she made an appointment with me, an Addictions Counselor, for a form of Aftercare. The pain remained, she had addictive tendencies, and she didn’t want to relapse – these were issues we could address.
I began the first session by building rapport: relying on cues gained from her eye movements and predicate phrases. Her statements “I feel like I have no control,” “I catch myself wanting to take a pill often during the day,” and “I have racked my brain trying to find ways to distract my thinking” indicated a K or a kinesthetic representation. So, I used similar words such as, “you must feel overwhelmed” and “the burden must be heavy,” as well as, mirrored the pace and tone of her speech, which was rapid and soft.
The Outcome Specification process, which I typically use, provided an understanding of what Josie wanted to achieve. Her responses were as follows:
1. What do you want?
JOSIE: I want to be prescription and over-the-counter medication free- even though I feel pain.
2. How will you know when you have reached the goal?
JOSIE: My goal will be reached when I no longer find reasons to take pain pills. I was at a point where I couldn’t go a couple of hours without them.
3. Where will the goal be relevant and/or irrelevant?
JOSIE: The goal will be relevant for me and my family. I don’t like taking pills, they upset my stomach, and I am not really there for my children or able to take care of my responsibilities because I am so sleepy and unmotivated after taking them. My husband is deployed, I am in charge; so, I must be strong – and I’m not.
4. What stops you from pursuing the goal wholeheartedly?
JOSIE: I am afraid that I won’t be able to manage the pain or my life without them.
5. What personal resources can you use to help achieve this goal?
JOSIE: My will is strong once I make my mind up to do something, I have been a military wife for ten years, and my family supports me.
6. What additional resources will you need to achieve the goal?
JOSIE: I need effective pain management techniques and help with my responsibilities. The kids, the house, my work, and my online classes –it is overwhelming.
7. How might the pursuit of the goal affect important people in your life? Is there any risk associated with achieving this goal?
JOSIE: My family will be relieved and I’d have more money and energy. Medications are costly and they make me sick. The risk is that I will start using them again.
8. What are daily actions you will need to take in order to achieve your goal? What is the first step?
JOSIE: I have to delegate some of my responsibilities b) I want more time for me, and c) I need effective non-medicinal ways to relive the pain.
FIRST STEP: Finding pain management strategies which do not include prescription or OTC medications.
9. Given everything you have considered to this point, is achieving the goal worth it? JOSIE: Absolutely!
Reviewing Logical Levels with A Client
I also reviewed the Logical Levels with Josie – identifying blocks and determining at what level it would be most effective to intervene. Her answers were as follows:
- Environment – taking meds at home when and where no one could see her.
- Behavior – an excessive reliance on prescription and over the counter drugs to ease pain and feelings of being overwhelmed.
- Capabilities –pills were available and no one knew she was taking them; they helped manage the pain and gave her strength to go forward each day.
- Beliefs – I should be able to cope like I did during other deployments. I must be strong. The meds make life bearable and they are legal. I am not hurting anyone.
- Identity – I am a military wife and military wives are strong – they always figure out how to cope. This family is solely my responsibility while my husband is deployed.
One option was to intervene at the environment level – not having medications available and having a friend to call when feeling overwhelmed. Knowing that each level builds on the ones below, I chose to focus on the Identity Level using Meta Model Questions to address deletions, distortions, and generalizations, “shoulds”, “musts”, and “can’ts.” Examples would be, “what would happen if the family wasn’t solely her responsible? Why does she have to be strong? and “Military wives always know how to cope?”
NLP Strategies I used
There are many ways to proceed; these are the NLP strategies that we used:
1. I taught Josie to dissociate from the pain by picturing it as far away, small and grey – seeing it as if she were watching a movie.
2. I guided her in creating an anchor – encouraging her to think of a time when she was pain free; then, anchoring that memory by grasping her left wrist with her right hand. We practiced several times until she felt the anchor was strong. When the pain arose, she was to use the anchor – taking her mind off the pain and onto a pain free time.
3. I instructed Josie to chunk down her list of responsibilities to a manageable size – spacing tasks throughout the day and delegating some as she regained strength.
4. In walking Josie through the Six Step Reframe, her answers were:.
………………. ……… a. The problem behavior was a compulsion to take medications.
………………………… b. The positive intent was to relieve pain and stress.
………………………….c. Yes – to alternatives
………………………….d. Brainstorming ideas included taking breaks, finding hobbies, joining a fitness club, and hiring a babysitter; as well as, getting massages and enrolling the boys in a sports program.
………………………….e. Her three choices were: joining a fitness club, getting massages, and enrolling the boys in sports programs.
………………………….f. She had no objections, but was afraid she would fail.
………………………….g. She agreed to move forward on the three choices and promised to update me on her progress the next time we met.
5. I taught Josie to alter her thinking process as she chose to take the medications. Typically, when she felt overwhelmed or was in pain, she pictured a bottle of pills, told herself how much better she would feel once she took the pill, imagined opening the cabinet and reaching for the pill bottle. This was a V-A-V strategy. So, I changed the pattern. When she felt the stress or pain, I had her picture the massage therapist working on her tight muscles, feel the muscles relaxing, and say how proud she was to have made the different choice. This would be a V-K-A strategy. Using this pattern, she recalled other options than reaching for pills.
During this article, I provided Josie with several NLP strategies to use regarding her goal of abstinence: creating anchors, chunking down, dissociating, and using a different thought pattern. I wanted her to determine which ones would be most effective as we delved into the deeper issues of why she thinks she will fail, why she needed to be so responsible and possible psychological attachments she may have. There is much to be done.
NLP Strategies for addiction treatment questions
We hope you found this article helpful and educational. If you have any questions regarding NLP Strategies counselors can use in the treatment of addictive behavior in individuals, we welcome you to post them in the designated section below. We try to answer all legitimate inquiries personally and promptly.
Related Posts